CNB is usually accomplished as the first biopsy modality. A14-gauge needle is inserted via a small puncture wound into the palpable mass directly or with the guidance of CT (Computed Tomography) or ultrasound. The needle insertion site should be in the line of the definite surgical incision (Figure 1).
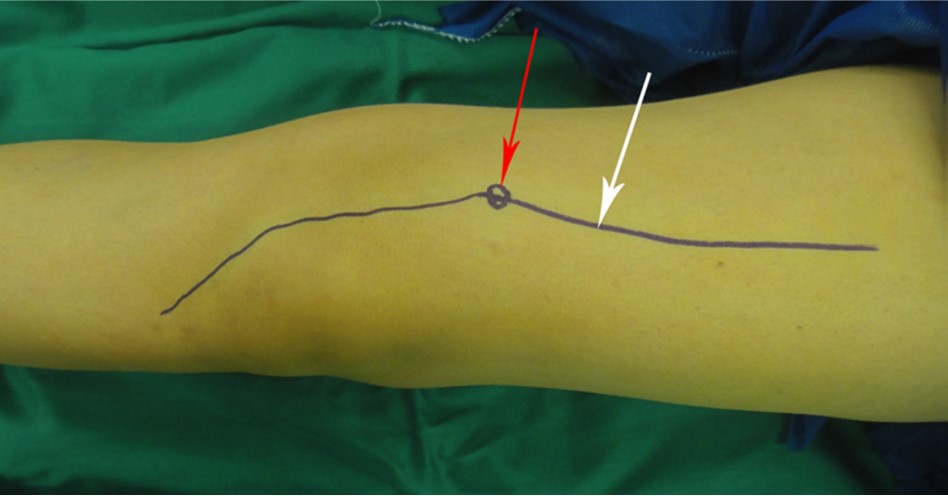
Figure 1. Photograph of the Planning for Core Needle Biopsy From the Distal Femur With Medial Bump. The definite surgical incision (white arrow) is designed for excision of biopsy
tract (red arrow).
Multiple cores in different didirections should be obtained. It provides a core of tissue with a 2 mm diameter and a maximum length of 20 mm .
The architecture of tissue is well preserved for histological diagnosis and ancillary analysis. Open biopsy is performed when the sample is not representative. It is useful for deep-seated lesions like the pelvis and spine and is performed under CT guidance. Less morbidity and fewer complication rates have been reported for percutaneous biopsy ranging between 0% and 17%, most commonly hematoma, bleeding, and infection. the interpretation of imaging studies has to be performed as the last procedure of diagnosis. Furthermore, staging studies determine the appropriate approach to the tumor and indicate which part of the tumor is representative. It should be performed with a frozen section to ensure appropriate tissue is obtained. If a benign diagnosis is confirmed, definite surgery can be completed in the same stage. It is best to use the smallest longitudinal incision compatible with obtaining adequate samples. The samples should be taken from the periphery of the tumors because of frequent central necrosis. Hematoma formation in biopsy wounds increases the risk of local spread of the tumor cells and logically increases the rate of local recurrence. A tourniquet should not be used routinely for this procedure because the bleeding vessel is hardly seen, and hemostasis is difficult to achieve. If a tourniquet is used to exsanguinate the limb, wrapping with an Esmarch bandage is contraindicated because this may push the tumor cell into the proximal part of the limb and even to the bloodstream. Before wound closure, the tourniquet should be deflated to accomplish precise hemostasis. If the drain path is contaminated, it has to be excised. The entry of the drain should be positioned in the line of the incision and close to it, i.e., no more than 1 cm.
Jamshidi, Khodamorad, and Abolfazl Bagherifard. "Biopsy of musculoskeletal tumors; current concepts review." Journal of Research in Orthopedic Science 2.1 (2015): 0-0.https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=Biopsy+of+Musculoskeletal+Tumors%3B+Current+Concepts+Review&btnG=#d=gs_cit&t=1693482115220&u=%2Fscholar%3Fq%3Dinfo%3AfYshaYGoybMJ%3Ascholar.google.com%2F%26output%3Dcite%26scirp%3D0%26hl%3Den